

Introduction
The role of upfront autologous stem cell transplantation (ASCT) for multiple myeloma (MM) has evolved over the last three decades, with significant improvements in preparative regimen, supportive care, induction, and maintenance therapy. In this study, we evaluated the survival trends for MM after ASCT in the last 25-years.
Methods
We included all consecutive MM patients who underwent their first ASCT at our center between January 1990 and December 2015. The primary aim was to compare survival trends at different time points. Secondary aims were to evaluate the impact of age (<65 vs ≥ 65 years), cytogenetics (standard vs high), and ISS stage (I vs II vs III) on survival. Primary endpoints were 5-year overall survival (OS) and progression-free survival (PFS). Secondary endpoints were cumulative incidence of relapse (CIR) and non-relapse mortality (NRM). The Kaplan-Meier method was used to estimate OS and PFS. CIR and NRM were determined using the competing risks method.
Results
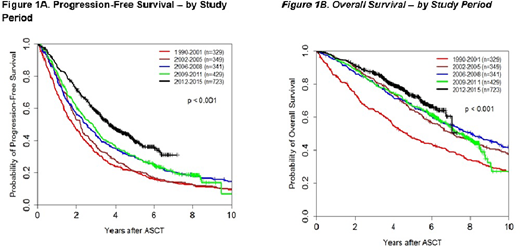
Overall, 2171 patients received their first ASCT during the study period. Median age was 58.5 (range: 23 - 82) years, 59% were males. Patients were subgrouped into 5 study periods, based on the years new therapies were approved and/or introduced in each period [specifically, the introduction of immunomodulatory drugs (IMiDs) and proteasome inhibitors (PIs)]: 1990-2001 (n=329; predominantly conventional induction chemotherapy), 2002-2005 (n=349; IMiD or conventional chemotherapy), 2006-2008 (n=341; IMiD or PI), 2009-2011 (n=429; predominantly PI over IMiD), and 2012-2015 (n=723; predominantly triplet therapy IMiD+PI, and majority received maintenance therapy). Compared to the 1990-2001 cohort (median age 52, range 22-71; 10% had ≥VGPR at ASCT), patients in the 2012-2015 cohort were older (median age 61, range 25-82) and had a deeper response at ASCT (≥VGPR: 49%). With a median follow up of 60.4 (0.2 - 302) months, the median PFS and OS and for all study patients were 32.4 and 89.5 months, respectively. There were significant improvements in PFS (HR [95%CI] 0.85 [0.83-0.88]; p<0.001) and OS (0.86 [0.83, 0.90]; p<0.001) trends over the study period. Median [95% CI] PFS and 5-year PFS improved from 1.8 [1.5-2.1] years and 21% in the 1990-2001 cohort, to 3.7 [3.3-4.1] years and 40%, respectively, in 2012-2015 (Figure 1A). Similarly, median [95% CI] OS and 5-year OS increased from 4.7 [3.9-5.6] years and 47%, respectively, in the 1990-2001 cohort, to not reached (NR) [7.0 years - NR] and 73%, respectively in the 2012-2015 cohort (Figure 1B). CIR improved with each subsequent study period, with 5-year rates of 68% in 1990-2001 and 56% in 2012-2015 (HR 0.88 [0.85-0.91]; p<0.001). Furthermore, a significant improvement in NRM was also noted, with decrease in 3-year NRM from 10% in 1990-2001 to 2% in 2012-2015 (HR 0.77 [0.69-0.87]; p<0.001).
In univariate analysis, significant improvements in PFS and CIR were noted across all patient subgroups with each subsequent study period. However, regarding the OS benefit, there was no significant improvements for age ≥ 65 years (HR 0.93 [0.82-1.05]; p=0.23) and ISS stage III (HR 0.94 [0.86-1.03]; p=0.18) subgroups. Patients with poor-risk cytogenetics had significant improvement, albeit remained with inferior outcomes relative to other subgroups; 5-year PFS and OS of 32% and 58% in 2012-2015, respectively, compared to 13% and 31%, respectively, in 1990-2001.
Conclusions
Survival outcomes for MM patients who underwent high-dose chemotherapy and ASCT have significantly improved over the last 25 years. The best outcomes were noted in the 2012-2015 cohort, which coincides with improvements in supportive care, IMiD + PI-based induction, and widespread use of maintenance therapy. Older patients (age ≥65 years), advanced ISS Stage III disease, and patients with high-risk cytogenetics, had less favorable survival and novel strategies to improve outcomes are needed.
Bashir:Celgene: Research Funding; Purdue: Other: Advisory Board; KITE: Other: Advisory Board; Amgen: Other: Advisory Board; Takeda: Other: Advisory Board, Research Funding; Acrotech: Research Funding; StemLine: Research Funding. Nieto:Secura Bio: Other: Grant Support; Novartis: Other: Grant Support; Astra Zeneca: Other: Grant Support; Affimed: Consultancy, Other: Grant Support. Mehta:Kadmon: Research Funding; CSL Behring: Research Funding; Incyte: Research Funding. Hosing:NKARTA Inc.: Consultancy. Ciurea:Kiadis Pharma: Current equity holder in publicly-traded company, Research Funding. Popat:Bayer: Research Funding; Novartis: Research Funding. Khouri:Bristol Myers Squibb: Research Funding; Pfizer: Research Funding. Kebriaei:Ziopharm: Other: Research Support; Novartis: Other: Served on advisory board; Amgen: Other: Research Support; Pfizer: Other: Served on advisory board; Jazz: Consultancy; Kite: Other: Served on advisory board. Manasanch:Takeda: Honoraria; GSK: Honoraria; BMS: Honoraria; Sanofi: Honoraria; Quest Diagnostics: Research Funding; JW Pharma: Research Funding; Adaptive Biotechnologies: Honoraria; Novartis: Research Funding; Merck: Research Funding; Sanofi: Research Funding. Kaufman:Janssen: Research Funding; Karyopharm: Honoraria; Bristol Myers Squibb: Research Funding. Patel:Celgene: Consultancy, Research Funding; Takeda: Consultancy, Research Funding; Precision Biosciences: Research Funding; Poseida: Research Funding; Oncopeptides: Consultancy; Cellectis: Research Funding; Janssen: Consultancy, Research Funding; Bristol Myers Squibb: Consultancy, Research Funding; Nektar: Consultancy, Research Funding. Shpall:Magenta: Membership on an entity's Board of Directors or advisory committees; Zelluna: Membership on an entity's Board of Directors or advisory committees; Celgene: Membership on an entity's Board of Directors or advisory committees; Novartis: Membership on an entity's Board of Directors or advisory committees; Adaptimmune: Membership on an entity's Board of Directors or advisory committees; Takeda: Other: Licensing Agreement. Lee:Celgene: Consultancy, Research Funding; Sanofi: Consultancy; GlaxoSmithKline: Consultancy, Research Funding; Amgen: Consultancy, Research Funding; Janssen: Consultancy, Research Funding; Daiichi Sankyo: Research Funding; Regeneron: Research Funding; Genentech: Consultancy; Genentech: Consultancy; Takeda: Consultancy, Research Funding. Orlowski:Laboratory research funding from BioTheryX, and clinical research funding from CARsgen Therapeutics, Celgene, Exelixis, Janssen Biotech, Sanofi-Aventis, Takeda Pharmaceuticals North America, Inc.: Research Funding; Amgen, Inc., AstraZeneca, BMS, Celgene, EcoR1 Capital LLC, Forma Therapeutics, Genzyme, GSK Biologicals, Ionis Pharmaceuticals, Inc., Janssen Biotech, Juno Therapeutics, Kite Pharma, Legend Biotech USA, Molecular Partners, Regeneron Pharmaceuticals, Inc.,: Honoraria, Membership on an entity's Board of Directors or advisory committees; Sanofi-Aventis, Servier, Takeda Pharmaceuticals North America, Inc.: Honoraria, Membership on an entity's Board of Directors or advisory committees; Founder of Asylia Therapeutics, Inc., with associated patents and an equity interest, though this technology does not bear on the current submission.: Current equity holder in private company, Patents & Royalties; STATinMED Research: Consultancy. Champlin:Johnson and Johnson: Consultancy; Cytonus: Consultancy; Actinium: Consultancy; Omeros: Consultancy; Genzyme: Speakers Bureau; DKMS America: Membership on an entity's Board of Directors or advisory committees; Takeda: Patents & Royalties. Qazilbash:Bioclinica: Consultancy; Amgen: Research Funding; Angiocrine: Research Funding; Bioline: Research Funding; Janssen: Research Funding.

